Entrustable Professional Activities (EPAs) are units of professional practice that represent the essential tasks physical therapists perform in daily clinical care. Because clinical education should mirror real-world practice, Marian University's DPT program uses an EPA-driven model to assess students on the activities they will routinely perform in the clinic.
Throughout their clinical experiences, students partner with clinical faculty to engage in ongoing assessment and meaningful feedback on their performance across the 19 EPAs. This collaborative process supports students in taking ownership of their professional development while progressively building the competence and trust needed for independent physical therapy practice.
Physical therapists provide patients or clients with information on the diagnosis, prognosis, treatment options, and risks and benefits of treatment options. Respecting patient and client autonomy in decision-making, “informed consent occurs when communication between a patient and provider results in the patient’s authorization or agreement to undergo a specific intervention.”
Physical therapists perform an initial examination of a patient or client that is comprehensive, consistent with and supported by evidence, and considers the individual factors and characteristics unique to the patient or client.
Performance of this EPA is predicated on the practitioner possessing the ability to perform a history, review of systems, and examination, including systems review and tests and measures accurately, as well as the knowledge of normative data to analyze and interpret outcomes.
Physical therapists establish a diagnosis for each patient or client encounter that reflects identified signs, symptoms, and/or impairments in body structures and function.Performance of the EPA is predicated on the ability to organize and interpret all relevant information that is part of the diagnostic process (obtaining relevant history, performing systems review, and selecting and administering specific tests and measures).
Physical therapists formulate a management plan that includes a plan of care. Performance of this EPA is predicated on the ability to obtain information through the history and physical exam to formulate a diagnosis. Developing a plan of care is an iterative process based on the best available evidence that requires synthesis of medical, ethical, legal, and economic factors, as well as knowledge of the strengths and limitations of the patient or client, physical therapist, team, and facilities.
Physical therapists implement a plan of care that is predicated on the development of a plan of care (by oneself or another physical therapist) that addresses problems and activity limitationsidentifiedthrough examination and evaluation.
Physical therapists select, prescribe, and implement interventions targeted toestablishedgoals and based on the available evidence, examination findings, diagnosis, andprognosis. Physical therapists must also adhere to the personal, professional, and jurisdictional scope of practice and institutional, state, and federal guidelines.
Physical therapists provide an evidence-based comprehensive home program based on a given patient’s or client’s presentation, symptoms, activitylimitationsand participation restrictions to address their stated goals of rehabilitation. This program considers health promotion and wellness needs, the patient’s or client’s goals, comorbidities, available resources, and stage of healing. Instructions are provided in theappropriate mode(written or electronic) at alevelcommensuratewith the patient’s or client’s preferred learning style, language, and education level.
Physical therapists are accountable to provideaccurate, focused, and context-specific documentation of each patient or client encounter in either written or electronic formats. The patient or client record is a legal document that is a critical form of communication that supports the ability to provide continuity of care to patients or clients.
At any point in an episode of care, or in a long-term or ongoing physical therapist-patient or client relationship, a physical therapist may use the knowledge from assessments performed to refer patients and clients to other professionals when they require intervention or assessment, including the need for emergent care. This may include consultation with or referral to other health care professionals or a physical therapist colleague with advanced expertise, or additional postprofessional education or certification (eg, board-certified clinical specialist).
Physical therapists inform, educate and train others, including patients and clients, caregivers, communities, families, significant others, and other health care providers, as acomponentof practice. The physical therapist teaches in a way that can be appreciated bythe learners (eg, cognition, knowledge, language) and considers domains of learning (cognitive/knowledge, psychomotor/skills, affective/attitudes).
Physical therapists supervise physical therapist assistants, aides, technicians, and junior learners (eg, high school/college/PT students). Proper supervision ensures safeand effectivedelivery of physical therapy services. The physical therapistmaintainsresponsibility for patient and client management at all times, consistent with jurisdictional rules and laws governing supervision.
Physical therapists assess and interpret the outcomes of a plan of care and determine whether continued physical therapy is indicated or if the patient's episode of care should be concluded. Performance of this EPA is predicated on the practitioner possessing the ability to relate the patient's current ability and performance to normative data while considering results of the evaluation and all established goals.
The physical therapist concludes an episode of care (ie, discharge, transition) when the goals and outcomes for the patient or client have been achieved, when the patient or client is unable to further progress toward goals, or when the physical therapist determines that the patient or client will no longer benefit from physical therapy. Conclusion of a single episode of care may not, in some circumstances, signal the end of a patient- or client-provider relationship (ie, the patient may continue services for another diagnosis).
Physical therapists, in collaboration with the patient or client, determine discharge recommendations for a patient or client that are supported by evidence and individual outcome data from the patient or client encounters and consider the individual factors and characteristics unique to the patient or client. This recommendation may include optimal settings for physical therapist services and equipment needed by the patient or client.
Physical therapistsidentifyopportunities for improvement within all aspects of care,identifypatient safety incidents, and offer solutions to address them. All care situations involve chances for errors to occur that can affect the patient’s health or the course of care.Identifying, responding to, analyzing, documenting, and addressing avoidable process failures is important to protect and promote patient safety.
Physical therapists' roles in prevention and promotion of health, wellness, and fitness range from encouraging healthy behaviors in individuals without conditions to helping individuals with chronic conditions engage in physical activity. Physical therapists conduct screening(s) to determine the need for primary, secondary, or tertiary prevention services; further examination, intervention, education, or consultation by a physical therapist; or referral to another practitioner.
The physical therapist evaluates access to services andutilizesbilling procedures thatare in compliance withgoverning rules and regulations, and consistent with the ethics of the profession.
The application of systematic triage systems in the delivery of therapy services to patients whilemaintainingthe highest level of quality is essential. A physical therapist recognizes and triages services based on resources, patient need, urgency, and complexity.
Effective and efficient handoff communication is critical for patient care. Handoff communication ensures that patients continue to receive high-quality and safe care through transitions of responsibility from one health care team or practitioner to another. Handoffs are also foundational to the success of many other types of interprofessional andintraprofessionalcommunication, including discharge from one provider to another and from one setting to another. Handoffs may occur between settings (eg, hospital to outpatient/homecare; pediatric to adult caregiver) or within settings (eg, floor to ICU; day treat to outpatient, inpatient rehab to day treat; school system to outpatient).
Physical therapists often are the first health care providers toinitiatephysical activity, assess patient response to movement, move with a patient, stress the cardiac system, and maywitnessa patient decompensate or have asignificant changein status. The ability to promptly recognize a patient whorequiresurgent or emergent care, initiateevaluationand management, and seek help is essential. Physical therapists may be theinitialhealth care provider to recognize a change in a patient’s status during these events in any setting. Early recognition and interventionprovidethe greatest chance foroptimaloutcomes in patient care. This EPA calls for simultaneously recognizing the need andinitiatinga call forassistance.
Clinical Education Curriculum
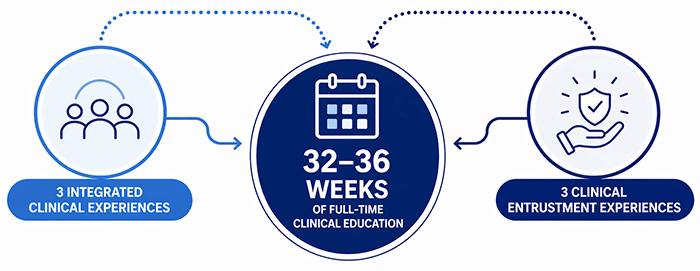
The DPT clinical education curriculum consists of two types of learning experiences: Integrated Clinical Experiences and Clinical Entrustment.Students willparticipatein part-time and full-time experiences to engage with various practice settings, life spans, and diagnoses.
Integrated Clinical Experiences
Integrated Clinical Experiences (ICE) introduce students to real-world physical therapy practice through supervised clinic visits that are integrated throughout the early part of the curriculum.
Progressive learning: Across three experiences, students build and apply skills in patient examination, intervention, documentation, clinical reasoning, and patient education.
Collaborative mentorship: Students work closely with clinical instructors to apply classroom learning in authentic patient care settings.
EPA development: These experiences provide early opportunities to practice skills aligned with Entrustable Professional Activities (EPAs) while reinforcing professionalism, ethical practice, and patient-centered care.
Clinical Entrustment
Clinical Entrustment (CE) experiences provide extended, full-time clinical placements where students apply and refine their skills in real-world physical therapy practice under the supervision of clinical faculty.
Progressive responsibility: Across three experiences, students build toward increasingly independent practice as they perform patient examination, develop and manage plans of care, and implement interventions.
Developing clinical autonomy: Students strengthen clinical reasoning, decision making, communication, and professional behaviors while contributing meaningfully to patient care.
EPA Entrustment: Through ongoing assessment and feedback, students demonstrate trustworthiness in performing the 19 EPAs, ultimately achieving the level of independence expected of entry-level physical therapists.
Flexible Timeline: Students who achieve early EPA entrustment may complete the final clinical experience in 10 weeks and participate in a Capstone elective designed to support advanced professional identity formation.
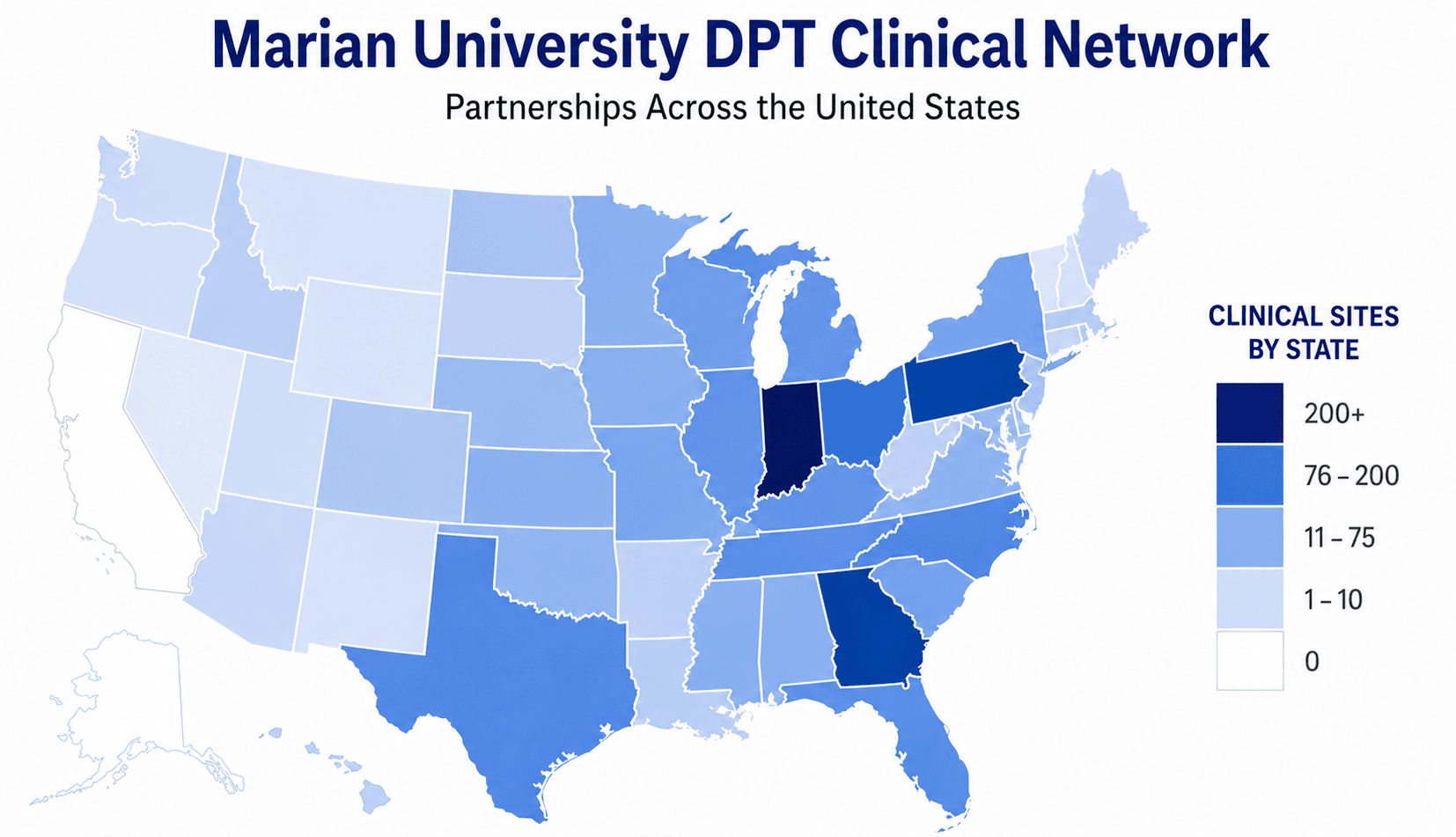
Marian University collaborates with clinical partners across the country to provide a variety of high-quality learning experiences for its students. Students should expect to travel outside of the Indianapolis metropolitan area during at least one Clinical Entrustment experience.
DPT Admission Info
(317) 955-6400 GRAdmissions@marian.edu
Program-Specific Info
Stephanie Miller, PT, Ph.D. Program Director and Professor (317) 955-6310 smiller1@marian.edu
Graduation from a physical therapist education program accredited by the Commission on Accreditation in Physical Therapy Education, 3030 Potomac Ave., Suite 100, Alexandria, VA 22305-3085; phone; 703-706-3245;accreditationsupport@apta.orgis necessary for eligibility to sit for the licensure examination, which is required in all states.
Candidacy is considered to be an accredited status, as such the credits and degree earned from a program with Candidacy status are considered, by CAPTE, to be from an accredited program. Therefore, students in the charter (first) class should be eligible to take the licensure exam even if CAPTE withholds accreditation at the end of the candidacy period. That said, it is up to each state licensing agency, not CAPTE, to determine who is eligible for licensure. Information on licensing requirements should be directed to the Federation of State Boards of Physical Therapy (FSBPT;www.fsbpt.org) or specific state boards (a list of state boards and contact information is available on FSBPT's website.
Marian University is seeking accreditation of a new physical therapist education program from CAPTE. On April 30, 2026 the program submitted an Application for Candidacy, which is the formal application required in the pre-accreditation stage. Submission of this document does not assure that the program will be granted Candidate for Accreditation status. Achievement of Candidate for Accreditation status is required prior to implementation of the professional phase of the program; therefore, no students may be enrolled in professional courses until Candidate for Accreditation status has been achieved. Further, though achievement of Candidate for Accreditation status signifies satisfactory progress toward accreditation, it does not assure that the program will be granted accreditation.